Oral Health Country/Area Profile Project
Palestine - Integrating the WHO Health Promoting School Concept into National School Oral Health
Palestine - Integrating the WHO Health Promoting School Concept into National School Oral Health
Dr Lamis Abuhaloob WHO CC for Public Health Education and Training, Imperial College London, London, United Kingdom
Professor Poul Erik Petersen WHO Collaborating Centre for Community Oral Health Programmes and Research, University of Copenhagen, Denmark
Introduction
The Palestinian Territories comprise two geographically separated areas (Figure 1): West Bank (WB) and Gaza Strip (GS). The WB comprise an area of 5,800 km2 west of the River Jordan. The GS is a narrow strip of highly populated land of 360 km2 lying on the eastern coast of the Mediterranean Sea1. The WB and GS contain 16 and 7 governorates, respectively2.
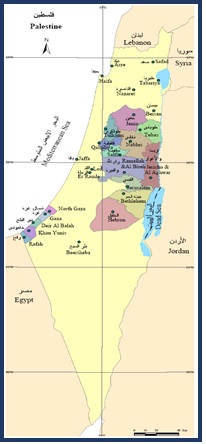
Figure 1. Map of Palestinian Territories
The long-term political instability in the Palestinian territories has caused serious deterioration of socioeconomic conditions. In addition, because of financial limitations existing health services are unable to meet the population’s oral healthcare3. This is the first national oral health promotion study in Palestine applying the principles of the WHO Health Promoting Schools concept4 at the national level and involved representative governmental primary schools from all governorates.
Project Outline
A quasi-experimental study (2016-2018) recruited 3939 schoolchildren aged 5-6 years from 30 intervention schools (n=2333) and 31 comparison schools (n=1606). At baseline and post-intervention, mothers and schoolteachers completed WHO self-administered questionnaires about the oral health of children, oral health behaviour, and family factors. A total of 25 calibrated dentists examined the dental caries of children according to WHO criteria. Trained teachers in the intervention schools provided comprehensive oral health education to children in the classrooms, held regular oral health sessions for mothers, and supervised children's daily toothbrushing with fluoride-containing toothpaste (1,450 ppm F) at school.
The project implementation process is summarised in Figures 2, 3, 4, 5 and 6.
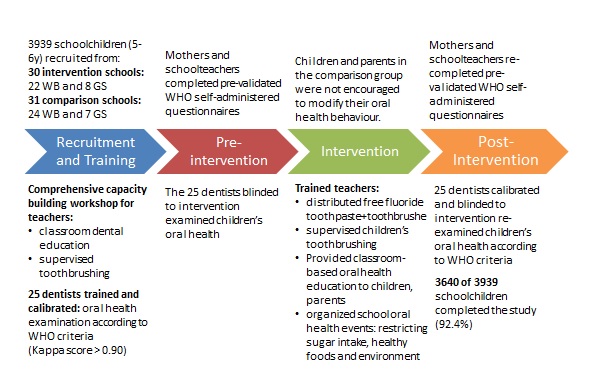
Figure 2. Chart describing Palestinian school oral health project implementation process
Figure 3: Teachers’ capacity building and dentists' training workshops in the Ministry of Health and Ministry of Education in Palestine
Figure 4. School oral health dentists examine Palestinian children’s oral health based on the WHO criteria


Figure 5. Trained teachers provide classroom-based oral health education to children and parents in Palestine


Figure 6. Trained teachers distribute fluoride toothpaste and toothbrushes free of charge and supervise children’s daily toothbrushing
Achievements
After 24 months of the programme implementation, the follow-up was completed for 75.8% of recruited children. The results showed that dental caries experience declined over the project, in both dentitions. The reduction in DMFT and DMFS was 23.3% and 23.2% (P<0.001), respectively. The drop-in caries experience indices in Gaza Strip were four to eight times higher than in West Bank and reached a 47.4% reduction in DMFT (Figure 7)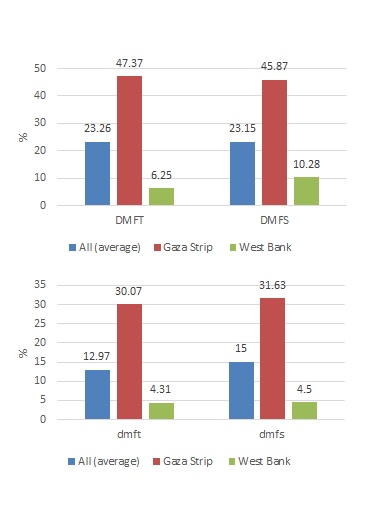
Figure 7. Reduction (%) in dental caries experience of schoolchildren in intervention collaborative schools compared to control schools (P<0.001)
In the intervention group, fewer children avoided smiling, fewer children missed classes because of toothache and 40% of children visited a dentist once or twice a year. The main reason for visiting the dentist was pain/troubles with teeth or gums. The percentage of children practicing toothbrushing at home two or more times a day increased, and 72.5% of the children used fluoride-containing toothpaste.
For 76.9% of 6-years old schoolchildren in the intervention schools, parents were the main source of information on oral healthcare. The contribution of teachers to oral healthcare facts raised to 43.3% in the intervention group by the end of the study (Figure 8).
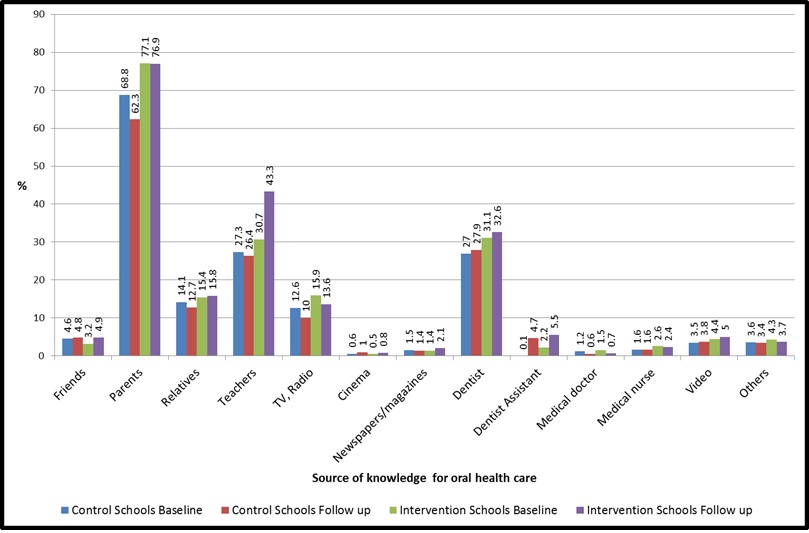
Figure 8. Source of knowledge for oral health care for 5-7-years old schoolchildren, at baseline and after 24 months
Mothers and teachers showed improvement in knowledge and positive attitudes towards dental care. The involvement of schoolteachers in oral health in schools and acceptance of dental health education materials significantly enhanced children’s oral health behaviour.
The WHO school oral health promotion programmes implemented in primary schools in Thailand10 and China11 showed a similar outcome.