Oral Health Country/Area Profile Project
United Kingdom - Childsmile – the national child oral health improvement programme for Scotland
United Kingdom - Childsmile – the national child oral health improvement programme for Scotland
INTRODUCTION
“Childsmile” is a national programme designed to improve the oral health of children in Scotland and reduce inequalities both in dental health and access to dental services. It is funded by the Scottish Government (Macpherson et al 2010). It commenced as pilots in 2006, and since 2011 has been delivered as an integrated programme in all Health Board areas throughout Scotland.“Childsmile” is a complex public health intervention and aims to adopt a common risk factor approach, recognising the importance of multidisciplinary and multi-settings approaches – integrating oral health with other groups and agencies. The programme also follows the principles of the national approach in Scotland for supporting the wellbeing of children and young people and improving outcomes by offering the “right help at the right time from the right people.” This is known as Getting it Right for Every Child (GIRFEC) and supports young people and their families to work in partnership with the services that can help them (Scottish Government 2017).
BACKGROUND AND RATIONALE
In the United Kingdom trends in children’s dental caries declined rapidly from the 1970s to the late 1980s, attributed to the introduction and widespread use of fluoride toothpaste during this period. However, by the 1990s, these improvements had begun to slow in Scotland, with children having among the worst rates of dental decay in the UK and Europe. Inequalities in dental decay were also becoming apparent, with those from the lowest socio-economic groups bearing the greatest burden.
The Scottish Government and National Health Service (NHS) Scotland are at the forefront of child oral health improvement. In response to the trends outlined above, the government commenced funding a nationwide universal supervised nursery toothbrushing programme in 2001.
An action plan for improving oral health and modernising NHS dental services in Scotland was published by the government in 2005 and this formed the basis for the development of the wider Childsmile programme, incorporating the established supervised toothbrushing intervention. The action plan included new investment for improving child oral health, and successive government administrations have continued to provide this funding.
PROJECT OUTLINE
The programme was designed and is evaluated using a theory-based approach. Logic models were developed following multi-stakeholder input. These identified the evidence-based health improvement activities which in theory were considered to be associated with long-term improved child oral health outcomes. Shorter-term service- and behaviour-change intermediate outcomes which would be required to achieve the health outcomes were also identified.
It is envisaged that every child in Scotland will, from birth, have access to “Childsmile”.
At a population level, every child will have access to:
• A tailored programme of preventive care within Primary Care Dental Services;
• Free daily supervised toothbrushing in the nursery (kindergarten) setting (aged 3-4 years);
• Free Dental Packs (toothbrush / 1450ppm fluoride toothpaste) to support toothbrushing at home.
Directed support targeting children and families in greatest need through:
• Community interventions involving home visits and links to public health nurses and community agencies and third sector organisations via dental health support workers;
• Clinical preventive programmes, involving fluoride varnish application, in priority* nursery and primary schools by extended duties dental nurses (age 3-8 years);
• Daily supervised toothbrushing in primary 1 and 2 classes (age 5-6 years) in priority* primary schools.
* priority nursery / school settings defined by children being from the most socioeconomically deprived communities.
Additionally, as part of a more upstream approach to health improvement, the programme is involved in advocacy for and involvement in development of national strategies and regulations relating to diet and nutrition.

Supervised Toothbrushing Programme:
- Every 3 and 4 year old child attending nursery (whether it is a local authority, voluntary or private nursery) is offered free, daily, supervised toothbrushing. Supervised toothbrushing closely follows national toothbrushing standards (Childsmile 2015) and the products (toothbrush and 1450 ppm F paste) are provided by a nationally procured contract to ensure consistency across Scotland.
- Supervised toothbrushing is also available to at least 20% of Primary 1 and Primary 2 classes (5-6 year old children) of schools situated in areas with the highest level of deprivation of NHS Boards across the country.
- To promote home brushing, every child is also provided with a Dental Pack (containing a toothbrush and a tube of 1450 F toothpaste) on at least six occasions by the age of 5. Children also receive a free-flow feeder cup by one year of age.
Fluoride Varnish in Nursery and School Programme:
- This delivers, via nursery and primary schools, the application of fluoride varnish to the teeth of children aged 3 to at least 8 years who are identified as living in the most deprived areas. It covers a minimum of 20% of children from each Health Board.
- Educational establishments are targeted in order of those with the highest proportion of children living in the most deprived local quintile as defined by the Scottish Index of Multiple Deprivation (SIMD) (Scottish Government 2016).
- Twice-yearly fluoride varnish applications are provided by “Childsmile” dental teams. The teams are composed of Extended Duty Dental Nurses (EDDNs) trained in the application of fluoride varnish and Dental Health Support Workers (DHSWs).
- At all stages in the programme, children who require further assessment and possible dental care are identified and their parents receive a letter informing them of their child’s dental need.
Community Interventions involving Health Visitors and Dental Health Support Workers:
Every newborn child in Scotland is linked to “Childsmile” via the universal child health surveillance system within the Universal Health Visitor Early Years Pathway (Scottish Government 2015) (Figure 1). Health Visitors see all children and their parents/carers on a regular basis between birth and 5 years. Health Visitors provide advice on oral health, distribute a Dental Pack, encourage dental attendance from a young age, and where they feel additional support may be required; they make a referral to a DHSW.
DHSWs (Dental Health Support Workers) provide the following:
Tailored support and advice in the family home
Linking to dental services and facilitating child attendance at a dental practice;
Signposting / linking to other community organisations and initiatives via social prescribing (e.g. community engagement, food co-operatives, infant feeding programmes).
For the most vulnerable families, a longer period of home support may be required before engaging with dental services.
Dental Primary Care:
There is encouragement for children to attend primary care dental services from six months of age. A programme of preventive care, tailored to meet the needs of the individual child, is provided by the dental team. This includes:
a) Oral health advice (e.g. on healthy weaning, diet, teething and toothbrushing instruction) and social prescribing if required;
b) Annual dental check-ups;
c) Twice-yearly fluoride varnish applications from two years of age.
Extended Duty Dental Nurses (EDDNs) within dental practices are trained in oral health promotion and fluoride varnish application to support the dental team to provide preventive care. As children age, there are opportunities for fissure sealant applications on first permanent molar teeth.
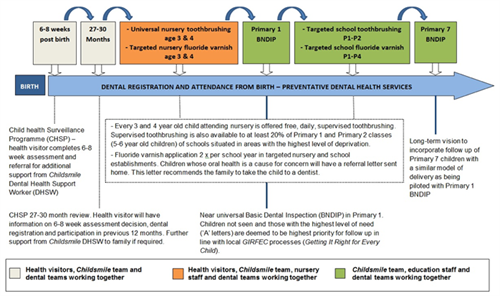
Figure 1. Childsmile Oral Health Pathway - illustrates the Childsmile’s distinct but integrated components, which extend from birth to adolescence. Source: Macpherson et al 2015
The National Dental Inspection Programme (NDIP 2017): is the national dental surveys of five-year-old (Primary 1 school year - P1) and eleven-year-old children (Primary 7 school year - P7). NDIP has two levels: a Basic Inspection (BNDIP, which all five-year-olds / eleven-year-olds receive each year), and a Detailed Inspection (dental epidemiological representative sample of five-year-old / eleven-year-old children in alternate years). BNDIP involves a simple assessment of the mouth of each child using a light, mirror and ball-ended probe. Each child is placed into one of three categories depending on the level of dental health and a letter sent to their parents, and pathways of ensuring children in high need receive appropriate dental care:
- Letter A (High Risk) – severe decay and should seek immediate dental care; or
- Letter B (Medium Risk) – some decay experience and should seek dental care in the near future; or
- Letter C (Low Risk) – no obvious decay but should continue to see the family dentist on a regular basis
ACHIEVEMENTS
Nationwide Coverage: “Childsmile” was piloted from 2006 and achieved population-wide national roll out in 2011. The programme has received strong and successive government commitment and funding (across three different political administrations).
Multi-setting and Multi-agency Working: A major achievement of “Childsmile” has been to develop and sustain buy-in from many stakeholders (Figure 2) – creating a broad coalition and collaboration with common goals. The programme has also been able to develop and deliver oral health improvement interventions outside of traditional dental clinical settings – into education establishments, community settings, other healthcare settings (integration to Health Visitor Early Years Pathway), and children’s homes.

Figure 2. Childsmile Stakeholder Map
Workforce Development:
Supported by NHS Education for Scotland (NES) – the national organisation for education and training in NHS Scotland – the “Childsmile” Programme has developed a highly skilled and trained workforce including extended duty dental nurses (EDDNs) and dental health support workers (DHSWs).
Dental nurses have been upskilled to apply fluoride varnish (in practice and nursery settings), and also deliver tailored oral hygiene toothbrushing instruction and dietary advice to parents/carers of young children.
Approval and changes to the dental regulations (via the General Dental Council) were sought and achieved to include fluoride varnish in the Scope of Practice of dental nurses.
“Childsmile” has also developed a new workforce group – the DHSW have been recruited, trained, and funded. They are embedded and work closely with health visitors, dental practices, and the Public Dental Service (who coordinate and administer the nursery and school components of the programme).
Changes to Primary Care Dental Contract: The “Childsmile”” Programme was involved in reorienting NHS primary care dental practices to be child friendly, and preventive focused. This involved incorporating Childsmile into the dental primary care contract (the Statement of Dental Remuneration SDR), with payments for preventive items of care including fluoride varnish, oral hygiene instruction, and dietary advice (Childsmile 2011).
Evaluation:
A strength of the programme is the integrated theory-based evaluation, led by the University of Glasgow, in collaboration with “Childsmile” stakeholders, and other academic partners, funded by the Scottish Government. This work is underpinned by a logic model and robust national data monitoring systems (including a bespoke “Childsmile” IT system developed by University of Dundee Health Informatics Centre (HIC)).
The evaluation research includes: i) a pioneering big data linkage project – linking multiple routine administrative national health and education datasets to create a birth cohort to evaluate the complex multiple interventions of “Childsmile” with the range of service and health outcomes; ii) an in-depth multi-faceted process evaluation – assessing the barriers and facilitators to the delivery of “Childsmile” programme and its components; iii) an economic evaluation – investigating the cost effectiveness of the programme and its components; and iv) an embedded randomised control trial of the nursery fluoride varnish programme – Protecting Teeth @ 3 trial (Wright et al 2015).
Outcomes:
Child Oral Health Improvement:
- The National Dental Inspection Programme (NDIP) data show substantial improvements in dental health or both 5- and 11-year-olds over time (NDIP 2016, NDIP 2017).
- More than two thirds (69%) of 5-year-old children had no obvious decay experience in their primary teeth in 2016 (d3mft=0) (Figure 3). This is a large improvement in comparison with 45% back in 2003, when NDIP started.
There has been a parallel continuing decline (improvement) in the mean number of decayed, missing and filled (dmft) primary teeth from 2.76 in 2003 to 1.21 in 2016.
Similar improvements are observed for 11 year olds – data from the latest survey demonstrates a decade of improvement from 53% with no obvious tooth decay in 2005 to 77% in 2017; and the mean D3MFT decreased from 1.29 in 2005 to 0.49 in 2017.

Figure 3. Trends in the proportion of 5 year olds with no obvious decay experience (dmft=0). Source: Information Services Division 2016 Nursery Toothbrushing:
A Scotland-wide population study aimed to assess the association between the roll-out of the “Childsmile” national nursery toothbrushing programme and a reduction in dental decay in five-year-old children (Macpherson et al 2013).
Figure 4 shows that before the start of the nursery toothbrushing programme (time, t = 0) the mean d3mft was increasing, and only after the programme commenced, did the mean d3mft begin to decrease. The results of the same study also showed that the slope of the uptake in toothbrushing was correlated with the slope in the reduction of d3mft (correlation = -0.64; -0.86, -0.16; p = 0.011). Thus, the improvement in the dental health of 5-year-olds was associated with the uptake of nursery toothbrushing.
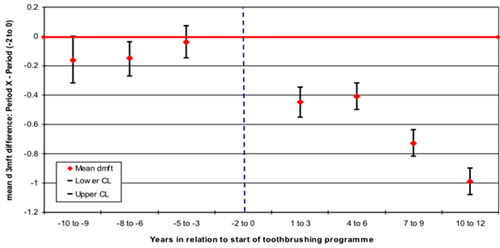
Figure 4. Mean d3mft for 5-year-olds in Scotland in relation to commencement of nursery toothbrushing
NOTE: Year 0 is a year before the start of nursery toothbrushing intervention (dotted vertical line). Period (-2 to 0) is a reference period.
Cost Analysis of Nursery Toothbrushing:
A recent study compared the cost of providing the Scotland-wide nursery toothbrushing programme with associated National Health Service (NHS) cost savings from improvements in the dental health of 5-year-old children: through avoided dental extractions, fillings and potential treatments for decay (Anopa et al 2015).
The study showed that the estimated cost of the nursery toothbrushing programme in Scotland was around £1.8 million per year. The estimated cost of dental treatments in the baseline year 2001/02 was just under £8.8 million, while in 2009/10 it was around £4 million. In 2002/03 the costs of dental treatments increased by 2.4%. However, in the following years the costs decreased dramatically with the estimated annual savings ranging from £1.2 million in 2003/04 (14% of costs in 2001/02) to £4.7 million in 2009/10 (54%). The NHS costs associated with the dental treatments for five-year-old children decreased over time. In the eighth year of the toothbrushing programme the expected savings were more than two and a half times the costs of the programme implementation (Figure 5).
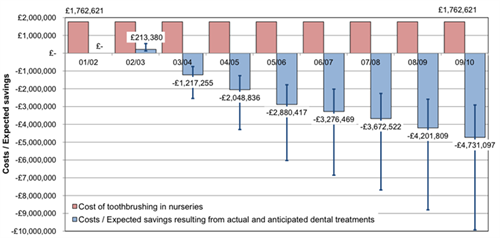
Figure 5. Annual cost of nursery toothbrushing programme and costs / expected savings resulting from actual and anticipated dental treatments in comparison with 2001/02 dental treatment costs. Source: Anopa et al 2015
Ongoing Challenges: Health inequalities remain a significant challenge. Figure 6 shows data from the NDIP report – the proportion of five-year-old children with no obvious decay experience by the Scottish Index of Multiple Deprivation (SIMD) quintiles (NDIP 2016). Quintile SIMD1 is the most deprived and quintile SIMD5 is the least deprived. Despite improvement in all groups, there are clear and persistent inequalities in child dental health over time, with only 55% of 5 year old children having no obvious decay experience in the most deprived areas compared with 82% in the least deprived areas.
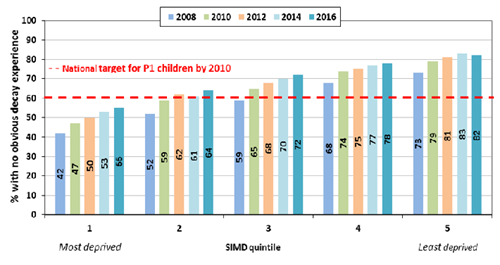
Figure 6. Proportion of Primary-1 children (five-year-old) with no obvious decay experience in Scotland by SIMD quintile. Source: Information Services Division 2016
CONCLUSIONS
The “Childsmile” programme has had significant achievements and been associated with major improvements in child dental health over time. However, socioeconomic inequalities persist, with children from the most deprived backgrounds bearing the greatest disease burden. A new national Oral Health Improvement Plan has recently been published (Scottish Government 2018) and sets the future direction for the programme to expand.
The future direction of the “Childsmile” programme includes: i) optimising the delivery of the existing programme through lessons learned from the evaluation, this will include a focus on vulnerable groups (e.g. children looked after by the state; McMahon et al 2017); ii) further community development work, this will include further work with the third (NGO) sector, social prescribing / linking with ongoing community-based initiatives; iii) influencing policy and programmes (“upstream”), including common risk work as part of the Non-communicable Disease (NCD) agenda (e.g. obesity / sugar strategy).
REFERENCES
Anopa, Y., McMahon, A.D., Conway, D.I., Ball, G.E., McIntosh, E. and Macpherson, L.M., 2015. Improving child oral health: cost analysis of a national nursery toothbrushing programme. PloS one, 10(8), p.e0136211.
Childsmile (2011). Incorporating Childsmile into the SDR. NHS Health Scotland http://www.child-smile.org.uk/documents/5475.aspx (Accessed Feb 2018).
Childmile (2015). National Standards for Nursery and School Toothbrushing Programmes. NHS Health Scotland http://www.child-smile.org.uk/professionals/childsmile-core/toothbrushing-programme-national-standards.aspx (Accessed Feb 2018).
Macpherson LM, Ball GE, Brewster L, Duane B, Hodges CL, Wright W, Gnich W, Rodgers J, McCall DR, Turner S, Conway DI (2010). Childsmile: the national child oral health improvement programme in Scotland. Part 1: Establishment and development. Br Dent J ;209(2):73-8.
Macpherson LMD, Anopa Y, Conway DI, and McMahon AD (2013). National supervised toothbrushing program and dental decay in Scotland. Journal of Dental Research 92(2):109-113.
Macpherson, L.M., Ball, G.E., King, P., Chalmers, K. and Gnich, W., 2015. Childsmile: the child oral health improvement programme in Scotland. Primary dental journal, 4(4), pp.33-37.
McMahon AD, Elliott L, Macpherson LM, Sharpe KH, Connelly G, Milligan I, Wilson P, Clark D, King A, Wood R, Conway DI (2017). Inequalities in the dental health needs and access to dental services among looked after children in Scotland: a population data linkage study. Arch Dis Child 103(1):39-43.
National Dental Inspection Programme (NDIP) 2016. Report of the 2016 Detailed National Dental Inspection Programme of Primary 1 children and the Basic Inspection of Primary 1 and Primary 7 children. Information Services Division, NHS Scotland. http://ndip.scottishdental.org/wp-content/uploads/2016/10/2016-10-25-NDIP-Report.pdf (Accessed Feb 2018).
National Dental Inspection Programme (NDIP) 2017. Report of the 2017 Detailed National Dental Inspection Programme of Primary 7 Children and the Basic Inspection of Primary 1 and Primary 7 children. Information Services Division, NHS Scotland. http://ndip.scottishdental.org/wp-content/uploads/2017/10/ndip_scotland2017-P7.pdf (Accessed Feb 2018).
Scottish Government (2015). Universal Health Visiting Pathway in Scotland – Pre Birth to Pre School http://www.gov.scot/Publications/2015/10/9697/0 (Accessed Feb 2018).
Scottish Government (2016). Scottish Index of Multiple Deprivation. 2016 Scottish Government. http://www.gov.scot/Topics/Statistics/SIMD (Accessed Feb 2018).
Scottish Government (2017). Getting it right for every child (GIRFEC) http://www.gov.scot/Topics/People/Young-People/gettingitright (Accessed Feb 2018).
Scottish Government (2018). Oral Health Improvement Plan http://www.gov.scot/Publications/2018/01/9275 (Accessed Feb 2018).
Wright W, Turner S, Anopa Y, McIntosh E, Wu O, Conway DI, Macpherson LM, McMahon AD (2015). Comparison of the caries-protective effect of fluoride varnish with treatment as usual in nursery school attendees receiving preventive oral health support through the Childsmile oral health improvement programme - the Protecting Teeth@3 Study: a randomised controlled trial. BMC Oral Health 15:160.
By LMD Macpherson, Y Anopa, J Rodgers, DI Conway