Oral Health Country/Area Profile Project
United Arab Emirates - MY SMILE” - tooth brushing program for school children in Dubai, UAE.
United Arab Emirates - MY SMILE” - tooth brushing program for school children in Dubai, UAE.
Introduction
Oral health has been a top priority in the Dubai Health Authority agenda for the strategy 2021. The main aim is to decrease the level of caries for children in Dubai, UAE. The latest data shows that the percentage of caries for children aged 5-6 years was 65%, which is considered higher than the average caries level in the region.(1)
The “MY SMILE” tooth-brushing program was introduced by Dr Shiamaa AlMashhadani in 2017 (2) under the direction and guidance of Dr Hamda AlMesmar, the Director of Dental Services Department of Dubai.
Background
The aim of the tooth-brushing scheme was to introduce forms of preventive activities that would decrease the high levels of caries prevalence among the students in Dubai schools. The tooth-brushing in schools scheme is an evidence-based intervention, drawing on principles and learning from comparable programs in Scotland (3), (4) and other research which show that the application of fluoride toothpaste in a supervised school-based intervention can have a significant effect on children with high caries risk. The tooth brushing program was designed with the intention of improving the oral health of young children and with emphasis on the importance of daily good oral hygiene habits (3).
Project Outline
“MY SMILE” tooth-brushing program
In 2017, “MY SMILE” program was introduced to 12 Government and Private schools in Dubai, covering 1500 students aged 4-6 years old. The implementation of the program required cooperation between the Ministry of Health and Prevention , the Knowledge and Human Development Authority ,School health and Educational Institute Unit, the private companies and Dental Services Department, Dubai Health Authority (2).
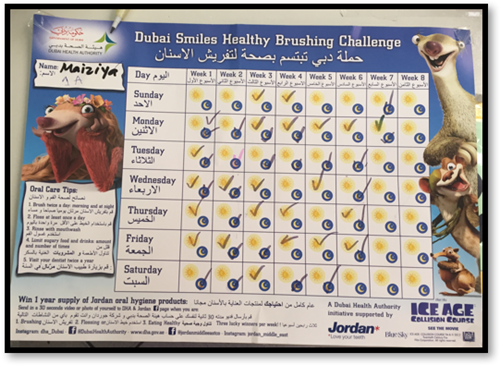
- Schoolchildren were provided with free toothbrushes appropriate for their age, fluoridated toothpaste and customized tooth brushing charts to record their daily tooth brushing.


- A training workshop was conducted for the oral health coordinators (school nurses) that were assigned to supervise the daily tooth brushing after meals and provide guidance and support to the students.
- Guidelines for tooth brushing in schools and infection control measures were adapted from the MySmile program (Scotland)(4) and copies provided to the oral health coordinators.

- The program involved two forms of tooth brushing based on the facilities in school.

Dry tooth brushing:
Schools that did not have the facility for children to go to washrooms to brush their teeth and spit excess toothpaste were given instructions to brush in their classrooms using appropriate amount of toothpaste and spit in cups or paper towels and were disposed of appropriately.


Wet tooth brushing:
Schools that had enough washrooms that accommodated the students were requested to take their tooth brushes with the proper amount of tooth paste and brush their teeth on the sink, rinse their tooth brushes and replace them back in the storages.
Toothpaste was placed on paper plates to help in infection control and enables the use of one toothpaste tube to be used for more than one student. (6)


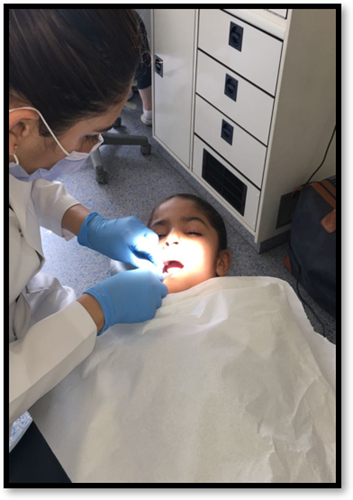
- A dental team of two dentists and two dental hygienists visited each school and conducted dental checkups using the visible plaque index (VPI) in a mobile dental van. Main concentration was to measure the plaque accumulation on the teeth surfaces for the students aged 4-6 years, as they were the age group with the highest caries prevalence based on the previous screening conducted in Dubai.
- Results were recorded for each student on oral hygiene forms and were placed in the student’s medical file in the school with the supervision of the school nurse.

- A visit to each classroom participating in the tooth brushing scheme was done with the presence of the of the school nurse (oral health coordinator) to check on the charts and tooth brushing storage facility.
- Parents were invited on the same day to have an introduction on the tooth brushing scheme and information given on healthy diet and good oral hygiene habits and tooth brushing charts were distributed to help them follow up on the brushing at home.

- Follow up from the dental team with oral health coordinator was done on a weekly and monthly basis.
- At the end of the three-month activity, a second dental checkup conducted on the students to record the dental plaque accumulation and compared with the previous results. An extensive interview was done with the oral health coordinator (school nurse and the feedback questionnaire from the parents were collected.
- An additional activity that encouraged children to be more involved with oral health was a drawing contest of healthy smiles, winners were given one year supply of tooth brushes and tooth paste to take home.

Outcome:
Data obtained from three resources, first dental surfaces that were free from plaque, secondly the interview with oral health coordinators in the schools and finally the feedback questionnaires from the parents.
Dental examinations for students involved in the brushing activity:
A total number of 1500 students were involved in the tooth brushing activity, parents consents for oral examination was obtained for the students aged 4-6 years only. Students were examined for plaque accumulation on teeth surfaces using The Visible Plaque Index (VPI). The index determines the frequency of tooth surfaces covered with clearly visible plaque (5), the outcome of which was dichotomized as “present” (at least one surface covered with visible dental plaque on the buccal region of the maxillary anterior teeth) or “absent” (dental plaque not visible on any surface of the buccal region of the maxillary anterior teeth). Scores were recorded on a screening sheet .The examination was done twice for the same students one before the tooth brushing activity started and the next one was after 90 days of continuous brushing in schools.
Associations between self-reported tooth brushing frequency and The Visible Plaque Index (VPI) was assessed using the chi-square test. Statistical analyses was performed with the aid of the SPSS Statistics™ program (SPSS for Windows, version 20.0, SPSS Inc., Chicago, IL, USA).
| Visible Plaque Index | Before tooth brushing in school n = 1000 (%) | After tooth brushing in school n = 1000 (%) |
| Present | 1,153 (76.8) | 551 (36.7) |
| Absent | 347 (23.2) | 949 (63.2) |
Table 1: Results of the examination in the number of dental surfaces free from plaque.
*Chi-square test
Interview with School nurses (oral health coordinators)
Interviews with the school nurses (oral health coordinators) involved a half hour interview with open-ended questionnaires related to:
• Commitment and support of the school administration in allowing students to do the tooth brushing at the assigned time on a daily basis,
• If the activity had fulfilled the learning objectives of the training, they had completed before the activity took place.
Another question was about their professional opinion if this activity contributed to children’s acceptance for daily brushing and interest in oral health.
• A set of questions were asked about the mechanism of the activity and the reactions of school staff in having students brush their teeth daily in the school.
• Any barriers that effect implementation of the tooth brushing activity.
In regards to the commitment of schools, 71% of the oral health coordinators responded that if the school administration enforced the activity the compliance was high both from the teachers and students, others informed that allowing students to take a ten minute break to brush their teeth and return back to the class was considered as a disruption to the students daily schedule.
A high response was to the questions about students’ reaction to brushing in school and how they considered it as an enjoyable task and made the students interested in brushing their teeth more often, even in schools that did not enforce daily tooth brushing students requested from their teachers to be given permission to brush their teeth.
Many of the Oral health coordinators (55%) agreed that the main barrier to have brushing as a daily activity in the schools was:
• Storage facility of the toothbrushes in the classrooms and maintaining infection control standards.
• Allowing students to leave the class to brush their teeth,
• The cooperation of the class teachers and the head administration to continue with the tooth brushing activity for a long period.
Parents Questionnaires:
Parents received a questionnaire to give feedback on their children experience with the tooth-brushing scheme. The questions asked about:
1-Did you receive information on the tooth brushing challenge from the school?
2-Would you consider tooth brushing in school for your child as a good way for her/him to establish good oral hygiene habits?
3- Have you noticed any positive behaviour change from your child towards tooth brushing at home?
4-How can the oral health team support you to enhance and encourage your children to maintain their good oral health habits.
□ Parents oral health lectures in school
□ Continue tooth brushing for children in school
□Any other suggestions ……………….
Parent’s feedback
Response rates for the feedback questionnaire was 95%.There was a high response rate for the positive behaviour change towards tooth brushing (86%). Many parents answered that the idea of their children brushing daily in school would help to establish a good oral hygiene routine (83%). They had increase interest to have more parents’ oral health sessions (72%). Most of the parents wanted their children to continue to brush at school (79%). There were 21% of parents who were concerned with infection control issues in regards to the storage of toothbrushes in schools.
Conclusion
The school-based oral disease preventive intervention comprised of oral hygiene instructions and supervised tooth brushing with fluoridated tooth paste(7) was effective in imparting oral health knowledge and establishing good oral hygiene habits in school children and in improving their oral hygiene status and the attitudes of their parents. With these positive findings, it is recommended that similar programs be supported and implemented with a larger sample size to determine the long-term effect of such programs and to improve the poor oral health situation among schoolchildren (8). Furthermore polices for such preventive methods should be placed to emphasis the importance of its effect and govern their implementation.
Acknowledgements
The author would like to thank Dr Hamda AlMesmar, Director of Dental Services Department , DHA for her kind support and guidance , Dr Wedad AlMaydoor and Dr Sara ALShaya from Ministry of Health and Prevention, UAE for facilitation of the program in the government schools. Dr Nusaiba Shaker from the School Health and Education Institutes unit for facilitation of private schools. Dental Services Department team of dentists (Dr Dana Iran, initiative leader of oral health awareness) and the team of dental hygienists in dental services department, Dubai Health Authority for their dedication and hard work.
Materials distributed to the students (toothbrushes, tooth paste and tooth brushing charts) were funded by Jordan ® and Philips®. There was no involvement of Jordan® and Philips® in the methodology and implementation of the study. We appreciate their support in the program.
by Dr Shiamaa AlMashhadani
Materials
Dubai Smiles Healthy School Practice
Dubai Smiles Healthy Child Health
Flip chart English
Flip chart Arabic
Dubai Smiles Healthy School Nurse Training
References
Shiamaa Shihab Al Mashhadani., et al. “National Survey of the Oral Health Status of School Children in Dubai, UAE”. EC Dental Science 8.2 (2017): 48-58.
Shiamaa Shihab Al Mashhadani. Tooth Brushing Schemes in Dubai Schools, A Step Forward in Oral Health Prevention. EC Dental Science 11.3 (2017): 88-94.
Macpherson L., et al. “National supervised toothbrushing program and dental decay in Scotland”. Journal of Dental Research 92.2 (2013): 109-113.
http://www.child-smile.org.uk/professionals/about-childsmile/childsmile-core.aspx
Satyawan G Damle., et al. “Effectiveness of supervised toothbrushing and oral health education in improving oral hygiene status and practices of urban and rural school children: A comparative study”. Journal of International Society of Preventive and Community Dentistry 4.3 (2014): 175-181.
An Evaluation of Calderdale’s Toothbrushing in Schools scheme James Woodall, Jenny Woodward, Karl Witty & Shona McCulloch
https://www.nice.org.uk/media/default/sharedlearning/797_toothbrushingevaluationreport_july2013final.pdf
Jackson RJ., et al. “The effects of a supervised toothbrushing programme on the caries increment of primary school children, initially aged 5-6 years”. Caries Research 39.2 (2005): 108-115
Curnow M., et al. “A randomised controlled trial of the efficacy of supervised toothbrushing in high-caries-risk children”. Caries Research 36.4 (2002): 294-300